-
Submissão Online Revisar Artigo
Rev. bras. psicoter. 2016; 18(2):92-114
Ferramentas
Artigos Originais
Clinical and Theoretical Considerations of Psychoanalysts and Cognitive Behavioral Therapists Regarding Generalized Anxiety Disorder in Argentina. A Qualitative Study of the Research-Practice Gap
Ignacio Etchebarne1; Santiago Juan2; Juan Martín Gómez Penedo3; Andrés J. Roussos4
Resumo
Este artigo apresenta dois estudos qualitativos que exploram a lacuna entre investigaçao e prática, como se relaciona com ao Transtorno de Ansiedade Generalizada, comparando as diferentes consideraçoes teóricas e clínicas da psicanalistas e terapeutas cognitiva-comportamentais de Buenos Aires.
MÉTODOS: No primeiro estudo, foram convidados um grupo de dez psicanalistas especializados e cinco terapeutas cognitivacomportamentais especializados para apresentar explicitamente a sua conceituaçao teórica desta desordem, com base nos critérios de diagnóstico da quinta ediçao do Manual Diagnóstico e Estatístico de Transtornos Mentais. No segundo estudo, vinte psicoterapeutas (dez de cada orientaçao teórica) foram convidados a ouvir uma gravaçao de áudio de um paciente fictício preenche os critérios diagnósticos de TAG e para apresentar sua impressao clínica sobre o caso. Através da análise qualitativa, as categorias foram criadas e avaliado após a sua frequência para ambos os estudos.
RESULTADOS/DISCUSSAO/CONCLUSOES: Os resultados mostraram semelhanças e diferenças em conceituaçoes teóricas e clínicas dos participantes e sugerem que as orientaçoes do terapeuta podem representar diferentes implicaçoes e obstáculos para superar a lacuna entre pesquisa e prática da psicoterapia.
Descritores: Transtornos de Ansiedade; Terapia Cognitiva; Terapia Psicanalítica; Características Culturais.Abstract
This paper presents two qualitative studies exploring the gap between research and practice, as related to Generalized Anxiety Disorder, by comparing the differing theoretical and clinical considerations of psychoanalysts and cognitive behavioral therapists from Buenos Aires.
METHODS: In the first study, a group of ten expert Psychoanalysts and five expert Cognitive-Behavioral Therapists were asked to explicitly present their theoretical conceptualization of this disorder, based on the diagnostic criteria of the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders. In the second study, twenty psychotherapists (ten from each theoretical orientation) were asked to listen to an audio recording of a fictional patient meeting GAD's diagnostic criteria, and to present their clinical impression about the case. Through qualitative analysis, categories were created and rated upon their frequency for both studies.
RESULTS/DISCUSSION/CONCLUSION: Results showed similarities and differences in participants' theoretical and clinical conceptualizations and suggested that therapist orientations may pose differing implications and obstacles to breach the psychotherapy research-practice gap.
Keywords: Anxiety Disorders; Cognitive Therapy; Psychoanalytic Therapy; Cultural Characteristics.
INTRODUCTION*
A BRIEF HISTORICAL ACCOUNT OF GAD
According to the fifth edition of the Diagnostic Manual of mental disorders (DSM-5)1, GAD is an anxiety disorder, characterized by the presence of chronic anxiety symptoms and pervasive worryness about various domains of everyday life, which produce clinically significant impairment. The estimates of the annual incidence and prevalence of GAD, locate it within the most prevalent anxiety disorders2. In comparison with other anxiety disorders present in the DSM editions, GAD seems to be a "newer" diagnosis, since it was the last to be included, as a valid entity in itself after a series of modifications to its criteria.
Etchebarne3 described how the Freudian notions of "Anxiety Neurosis" and "Anxiety Hysteria" (p. 217)4 were fused together in the DSM-I as an "Anxiety state" or "Anxiety reaction" (p. 32)5. Then, the name of "Anxiety Neurosis" was rescued in the DSM-II (p. 39)6, and only in the DSM-III was it reframed as a "Generalized Anxiety Disorder", separate from what we know today as "Panic Disorder" (p. 232)?7.
Across subsequent versions of the Diagnostic and Statistical Manual of Mental Disorders developed by the APA (the "DSMs"), GAD's categorical status and minimum duration have been modified, a shift from anxiety to worry as GAD's cardinal pathogenic agent has taken place, and a debate about its best denomination as an "anxiety" or "worry" disorder has been initiated8. As a result, GAD is the anxiety disorder that has undergone the greatest amount of modifications since its first publication in the DSM-III, in 19807, up to the DSM-5, in 20131.
Many authors have stated the need for improvement in the definition and understanding of this clinical problem2,9-11. As it will be described next, this situation is related to and has led to the development of multiple views regarding GAD's conceptualization.
DEBATES ABOUT CURRENT COGNITIVE-BEHAVIORAL AND PSYCHOANALYTIC CONCEPTUALIZATIONS OF GAD
With respect to GAD's Cognitive-Behavioral conceptualization, there is a general consensus in regarding excessive worryness as GAD's pathognomonic symptom2,10,12-14. Still, an ongoing debate is currently taking place about the role of worry in the maintenance of the disorder9,10,14,15. This has led to the development of multiple theoretical models of GAD that are derived mainly from the pioneering work of Borkovec and colleagues on the development of the "Cognitive Avoidance Model of Worry", who share the view that worryness serves some type of avoidance function10,14,15.
Describing each theoretical model of GAD exceeds the focus of this paper (for more information, see Behar's review9). Suffice it to say, a detailed analysis of each theoretical model presents an unfavorable situation with respect to GAD's conceptualization: Etchebarne3 has identified nine Cognitive-Behavioral theoretical models of GAD, that, taken together, signal nineteen maintenance factors for the disorder, and prescribe eight Cognitive-Behavioral approaches for GAD. It is unlikely that one mental disorder can have so many maintenance factors. For this reason, Etchebarne3 hypothesized the existence of an excessively high level of theoretical fragmentation and/or theoretical overlapping in GAD's Cognitive-Behavioral conceptualization.
Within the psychodynamic field, mainstream psychoanalysts sustain a somewhat paradoxical position since most reject the current diagnosis of GAD, regardless of its root in the Freudian notion of anxiety neurosis and anxiety hysteria16-18. Nonetheless, some psychoanalytic groups are beginning to accept GAD as a valid clinical entity in itself (Gabbard, 2000/2002). Examples of this recent tendency are Crits-Christoph and colleagues19,20, Ferrero and colleagues21, and Leichsenring and colleagues22, who studied the efficacy of psychodynamic treatments for GAD.
Some reconceptualizations of GAD phenomena have also taken place among psychodynamic authors. Crits-Christoph23 has reinterpreted Borkovec's theory about the avoidance role of worry in GAD24 in terms of the notion of unconscious defense mechanisms, locating GAD symptomatology within the Freudian psychoneuroses. Likewise, the Psychodynamic Diagnostic Manual task force (PDM)25,26 has included GAD within its diagnostic categories, but has conceptualized it as an anxious personality disorder, while explicitly excluding it from the anxiety disorders group. Based on these recent psychodynamic developments and classical psychoanalytical literature, Etchebarne3 has identified three psychoanalytic models of GAD symptomatology, six maintenance factors or disorder's dynamics, and four psychoanalytic approaches. In order to summarize this diversity, Table 1 summarizes Etchebarne's review3 of each theoretical model of GAD with its proposed maintenance factors or disorder's dynamics and therapeutic approaches:

METHODS
Given the several debates regarding GAD, we chose to conduct a qualitative research due to its capacity to approach topics from a perspective of openness to different voices and its ability to challenge, deconstruct, and hopefully, reintegrate prevailing therapeutic notions27. Likewise, we selected Consensual Qualitative Research (CQR)28-30 because it is an approach born within psychotherapy research that enables a rich and deep exploration of the phenomenon of interest while using a rigorous qualitative method31.
This project involved two separate studies with different interview protocols and groups of participants: a) the "Expert Study" and b) the "Stimulus Material Study". For this reason, we presented their respective methodology (sample characteristics, materials, and procedures), results and discussion separately, and, finally, integrated the results from the two studies into a general discussion.
THE EXPERT STUDY:
SAMPLE
A non-probabilistic, intentional sample was used for the present study, consisting of ten expert Psychoanalysts and five expert Cognitive-Behavioral therapists. Two criteria were established for identifying the therapists' theoretical orientation: 1) therapists labeled themselves as either Cognitive-Behavioral or Psychoanalytic, and 2) therapists were members of internationally renowned institutions or associations that specialized in their specific, self-labeled theoretical orientation. All participants were psychotherapists from Buenos Aires, Argentina.
To establish the condition of expertise in the sample we used an adaptation of Eells and colleagues' criteria32. In order to be defined as experts, therapists had to have had at least twenty years of clinical experience and meet one of these criteria: 1) having published several articles about Cognitive-Behavioral or Psychoanalytic theory and/or practice, 2) having published an innovation with respect to their therapeutic practice and/or theory, and 3) having conducted several workshops about their therapeutic practice and/or theory.
Only five expert Cognitive-Behavioral therapists participated in the study because such a target population is scarce in Argentina, since local certification in CBT by the Asociación Argentina de Terapia Cognitiva (AACT) only began in 200833. Demographic information of these 15 participants is shown in Table 2:

PROCEDURES
Individual semi-structured interviews (see interview protocols in Appendix A) were conducted with each participant in Buenos Aires, Argentina. Participants were contacted using a snowball method, and were explicitly asked about their theoretical conceptualization about what the DSM-5 defined as GAD1. All interviews were audio recorded after obtaining the informed consent from the participants and transcribed for codification.
Consensual Qualitative Research (CQR)28-30 was the methodology used for data analysis. This qualitative method requires the development of domains, core ideas, and categories derived from interview transcripts. Domains refer to each different topic area identified in the material, which are partially based on this study's research questions. Core ideas allude to the synthesis of minimal meaningful units of information, present in each domain, in each interview. Finally, the categories gather all similar core ideas across different interviews; i.e., they represent inter-subjective content (for an example of previous studies conducted with CQR by our research team, see: Etchebarne et al.34, Olivera, Braun, Gomez-Penedo, & Roussos35).
As prescribed for CQR28-30, generation of domains, core ideas, and categories for each framework sub sample was obtained by a process of consensus achievement through ongoing debate across the data analysis phase. Two advanced undergraduate psychology students comprised the primary analysis team, and two doctoral students functioned interchangeably as auditors. The team director served as a monitor during the entire process, supervising methodological concerns or obstacles, and served as a third-party discussant (with respect to the primary teams and auditors), during the interpretation of the results obtained throughout this study and the write up of this paper.
The developed categories were classified into General, Typical, or Variant, depending on their frequency of appearance across participants. Based on Hill and colleagues' indications29, in the expert psychoanalysts' subgroup we defined General as those categories identified in all the interviews within each subgroup of participants, or all but one. Typical categories included information identified in more than half of each subgroup up to the limit within the General frequency. Finally, Variant categories included information present in at least two cases, up to the limit within the Typical frequency. However, we had to change this frequency classification for the five expert Cognitive-Behavioral therapists interviewed, so as to maintain proportional equivalence with respect to the ten expert psychoanalysts' subgroup. Thus, a category present in all five interviews was considered General, in four or three, Typical, and in two, Variant.
In the discussion of this study, following Stile's suggestion for qualitative studies36, some Rare or Variant categories were also included because of their clinical relevance or peculiarity, which may also contribute to the generation of theory and future research.
As indicated by Hill, Thompson, and Nutt-Williams30, prior to the codification of the material, we discussed expectations and possible biases within the research team (Appendix D). These expectations presented must not be considered as formal research hypotheses of the study, but as a way of exposing researchers' previous theoretical assumptions, in an attempt to identify and limit the possible effect of conceptual biases during data analysis.
RESULTS
In this study three domains (topic areas) were identified: 1) GAD's diagnostic validity and delimitation, 2) GAD's theoretical conceptualization, and 3) functions and/or characteristics of worry in GAD. In Appendix B, examples of domains, core ideas, and categories developed for this study are shown.
GAD'S DIAGNOSTIC VALIDITY AND DELIMITATION
All five expert Cognitive-Behavioral therapists (CBTs) recognized GAD's diagnostic validity (General category), but they also underlined problems for the delimitation of the disorder (General category). On the other hand, seven out of ten Psychoanalysts (Typical category) stated that the notion of GAD was insufficient for a psychoanalytic conceptualization, while six out of these seven (Typical category) also stated that GAD was not a valid diagnosis.
GAD'S THEORETICAL CONCEPTUALIZATION
With respect to the theoretical conceptualization, in the CBTs' group, only Typical categories were observed (three out of five participants). This group of therapists referred to the role of temperamental vulnerabilities in GAD, the presence of meta-worries as a paradigmatic feature of the disorder, the proximity between GAD and depression, and the differentiation between generalized anxiety and personality disorders.
In the Psychoanalysts' group (Ps), two General categories were presented: nine out of ten participants conceptualized GAD in terms of its association with anxiety neurosis in particular, and/or actual neurosis in general. Eight of those nine participants, plus one other psychoanalyst, referred to GAD as being associated with psychoneuroses in general, and with anxiety hysteria in particular. Out of the first nine psychoanalysts mentioned, seven (Typical category) agreed that GAD can occur in different structures of the psychoanalytic psychopathology, and six participants (five of which were also included in the General categories) stated the possibility that GAD could imply a borderline or narcissistic disorder. We also observed that all Psychoanalysts associated GAD with at least two different features from the Psychoanalytic nosology.
FUNCTIONS AND/OR CHARACTERISTICS OF WORRY IN GAD
Finally, three out of five expert CBTs (Typical category) viewed worry as a cognitive avoidance mechanism, whereas two out of these three participants (Variant category) considered that worry in GAD could, in some cases, manifest itself as focusing momentarily on a single issue or problem.
Among the Ps, seven out of ten participants (Typical category) considered that worry in GAD could function as a defense mechanism, and three out of these seven (Variant category) added that worry in GAD could be understood as a displacement mechanism, more diffused than the one present in specific phobias. All CQR's results were synthesized into the following mind map (see Figure 1) to facilitate a holistic view of the obtained data within the Expert Group Study:

DISCUSSION FOR THE EXPERT STUDY'S RESULTS
GAD: A SPECIFIC DISORDER WITH AN UNRESOLVED DELIMITATION
Cognitive-Behavioral therapists (CBTs) accepted GAD as a clinical entity in itself and focused their discussion on its delimitation and nature. Unlike CBTs, almost all expert Psychoanalysts (Ps) rejected GAD as a clinical entity in itself. This can be partially explained by the historical reluctance of Psychoanalytic schools towards the use of the DSM descriptive system. However, it should be noted that despite their criticism of the validity of this diagnosis, Ps did identify some specificity of a patient potentially diagnosable with GAD, such as the defensive nature of worry or its association with neurotic or narcissistic structures.
CLINICIANS' VIEWS ABOUT THE FUNCTION OF WORRY IN GAD
It is worth noting that the issue of greatest consensus between the two expert subgroups (i.e., expert CBTs and expert Ps) consisted of considering worry in GAD as an avoidance or defense mechanism. This finding represents a convergent point not only between the two theoretical frameworks but also between clinicians and researchers on the understanding of GAD in general, and in relation to the role of worry in particular. Such convergence is also present in GAD publications, since, as mentioned in the introduction of this paper, the notion of worry as a cognitive avoidance mechanism24 has been incorporated by Crits-Christoph23, within a psychodynamic point of view, as a defense mechanism. Thus, this result further strengthens worry's theory as a maintenance factor in GAD. Nevertheless, the emphasis given to worry seems to depend on the theoretical orientation of the participant. For the Ps in this study, worry seemed to be just one of the many resistances they would have to neutralize so as to uncover hidden meanings in the patients' symptoms; while for the CBTs, disarticulating this pathological worry pattern and its associated beliefs clearly was their treatment's main goal.
GAD AS A PERSONALITY DISORDER: CLINICIANS SAY "NO"
It should also be noted that even though participants mentioned a relationship between GAD and certain personality traits or disorders (e.g., the role of temperament in the expert CBTs and the relationship with the borderline spectrum in the expert Ps), there were, however, few direct references alluding to GAD as a personality disorder in itself. Only one expert Cognitive-Behavioral participant and four expert Ps suggested this possibility. Psychoanalysts in the Expert Group did not tend to consider GAD as a personality disorder, even though this position is defended by the PDM Task Force25,26, as previously stated. Along the same line, some Cognitive-Behavioral researchers also advocate in favor of considering GAD as a personality disorder37-40 , while expert Cognitive-Behavioral participants disagreed.
THE STIMULUS MATERIAL STUDY:
SAMPLE
For the second study, a non-probabilistic sample was also used. In this case, it consisted of twenty psychotherapists, ten with Cognitive-Behavioral training and practice, and ten with Psychoanalytic training and practice. Participants in this sample had varying degrees of expertise. Table 3 shows the demographic data of these twenty participants.

The same previous criteria were established for identifying therapists' theoretical orientation: 1) therapists labeled themselves as either Cognitive-Behavioral or Psychoanalytic, and 2) therapists were members of internationally renowned institutions or associations that specialized in their specific, self-labeled, theoretical orientation. All participants were psychotherapists from Buenos Aires, Argentina. In relation to training, all participants were required to have specialized clinical training, supported or provided by the previously mentioned institutions.
MATERIALS
A 15-minute long audio recording of an adult fictitious patient, who met diagnostic criteria for GAD according to the DSM-51, developed by Etchebarne and Roussos41, was used as a Stimulus Material presented to the participants. This material has the format of a first interview with the patient talking in a continuous monolog, without any interviewer's intervention, and it was created from the GAD vignette published in the DSM-IV Casebook42.
PROCEDURES
Individual semi-structured interviews (see interview protocols in Appendix A) were conducted in Buenos Aires with each participant. We followed the same snowball method procedure described in the Expert Study. During the interviews, participants were asked to listen to the Stimulus Material and to present the patient's main problem and preliminary diagnosis. All interviews were audio recorded after obtaining the informed consent from the participants and transcribed for codification. Once again, CQR methodology28-30 was used for data analysis. Thus, information was coded into domains, core ideas, and categories, following the same steps described for the Expert Study.
RESULTS
Two domains (topic areas) were identified in the Stimulus Group study (n = 20). These were: 1) The patient's main problem identified in the Stimulus Material, and 2) The preliminary diagnosis for the Stimulus Material. In Appendix C, examples of domains, core ideas, and categories developed for this study are shown.
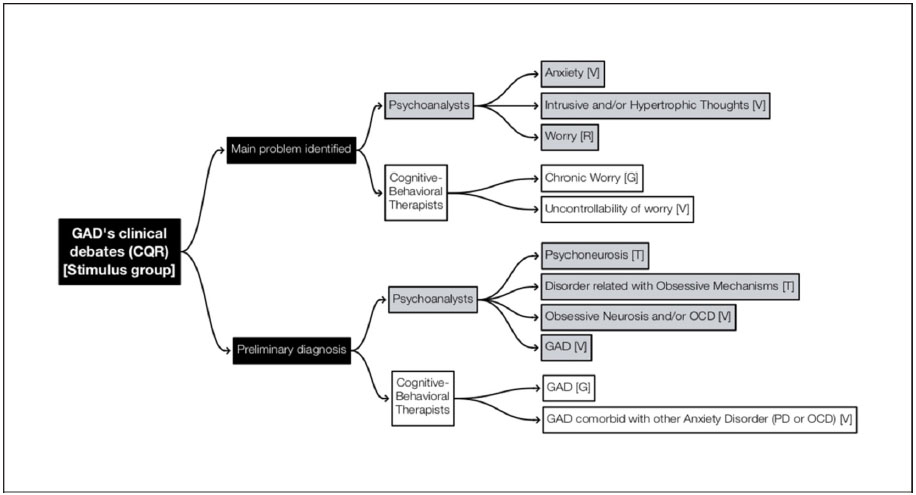
PATIENT'S MAIN PROBLEM IDENTIFIED IN THE STIMULUS MATERIAL
In the case of the CBTs, nine out of ten therapists (General category) identified chronic worry as the main problem, and three of those nine (Variant category) also stated the uncontrollability of worry as a central theme.
Unlike CBTs, for this domain, there were no General or Typical categories in the group of ten Ps, presenting only Variant categories (five out of ten participants). These categories referred to anxiety as the main problem, as well as the presence of intrusive thoughts. Only two subjects mentioned worry as a major problem.
PRELIMINARY DIAGNOSIS FOR THE STIMULUS MATERIAL
Regarding the preliminary diagnosis, all ten CBTs (General category) agreed on the diagnosis of GAD, while three of them (Variant category) proposed potential comorbidity between GAD and Panic Disorder and/or Obsessive Compulsive Disorder (OCD).
On the other hand, six out of ten Ps (Typical category) diagnosed the fictitious patient as presenting a prevalence of obsessive mechanisms and/or a psychoneurosis, and four out of these six (Variant category) spoke specifically about an Obsessive Neurosis or OCD. Results were synthesized into the following mind map (see Figure 2):

DISCUSSION FOR THE STIMULUS MATERIAL STUDY'S RESULTS:
ANXIETY VS. WORRY ROLE IN GAD: THE DEBATE GOES ON
The results obtained suggest that for the Stimulus Group, the Cognitive-Behavioral therapists considered worry as the axis of the clinical picture, while Psychoanalysts seemed divided, describing the main problem in terms of anxiety, hypertrophic/intrusive thoughts, or a combination of both. It is interesting to note that in their first studies about worry and insomnia, Borkovec and colleagues (p. 9)43 described worryness in terms of "obsessive worry" and as "an inability to turn off intrusive, affect-laden thoughts". In this sense, psychoanalysts who emphasized the patient's thought activity could also be attending to worry but conceptualizing it as an obsessive phenomenon. This difference in focus relates to the previously mentioned research debate regarding the place of anxiety and worry in the understanding of GAD. Each theoretical framework tended to identify a different clinical axis for GAD.
In the context of these results, we can hypothesize that the place of both anxiety and worry in GAD could be partially moderated by the therapist's theoretical orientation. While Psychoanalysis has traditionally aimed at clarifying the unconscious causes of the patient's suffering44, Cognitive-Behavioral therapists have generally considered causes as something aloof and, consequently, have prioritized the disarticulation of maintenance factors45. In this sense, worry is conceived as a maintenance factor to be changed by Cognitive-Behavioral therapists; whereas from a psychoanalytic perspective, anxiety has been conceptualized as a signal of activation of unconscious processes, i.e., something to be looked for because it "ignites" the discovery process of causes.
STIMULUS MATERIAL'S PRELIMINARY DIAGNOSIS: GAD, OBSESSIVE SPECTRUM DISORDER, OR BOTH?
With respect to the preliminary diagnosis for the Stimulus Material, we noted a much higher degree of consensus among CBTs than Ps. One reason for this might be the fact that Psychoanalysts' preliminary diagnosis was somehow divided among those who conceptualized the material from a Psychoanalytic perspective and those who used the DSM diagnostic criteria. CBTs applied only DSM descriptive psychopathology, and, in this sense, they all shared the same diagnostic grounding.
In spite of their lower consensus, the presence of the Obsessive-Compulsive Spectrum seemed crucial to the Psychoanalytic group when submitting a preliminary diagnosis. This diagnosis was not observed among the Cognitive-Behavioral participants, aside from some minor hypotheses of comorbidity with OCD. It could also be argued that these seemingly competing diagnoses are in fact displaying a multi-axial or multi-level diagnosis that enables the integration of both labels. While CBTs are clearly making an Axis I syndromatic or symptomatic diagnosis, psychoanalysts could be attempting a psychodynamic structural diagnosis, in which they relate GAD's symptoms to the obsessive spectrum, equivalent to an Axis II diagnosis of Obsessive-Compulsive Personality Disorder in DSM-51, though this association is not supported by epidemiological research2.
Finally, taking into account the fact that the Stimulus-Material was created from the DSM casebook42, making it a sort of "pure" GAD patient, it is interesting to note that comorbidity hypotheses appeared among some Cognitive-Behavioral participants. These results, summed up by the lower consensus presented by the Psychoanalysts, seem to indicate that GAD's diagnostic delimitation is also an unresolved issue among clinicians from different theoretical frameworks, and not only a researchers' debate. Thus, they reinforce the utility of this research dispute.
GENERAL DISCUSSION
THEORY, PRACTICE, AND EXPERTISE: A COMPARISON OF THE TWO STUDIES
We would like to discuss some differences observed between the Stimulus Study and the Experts Study. For instance, while the expert Ps rejected GAD's diagnostic validity, four out of the ten Ps from the Stimulus Group proposed GAD as a preliminary diagnosis. It is also striking that the presence of obsessive mechanisms and the relationship between GAD with Obsessive Neurosis was predominant in the Stimulus Group, but not in the Expert Group. These differences elicited from us the following questions:
On one hand, can such differences be explained by the fact that the Expert Group had to respond to an abstract theoretical task, while the Stimulus Group worked on a specific clinical case presentation? If this is the case, then these results would be confirming Alexander's assertion (p. 349)46:
"... authors' accounts about their theoretical views do not precisely reflect what they are actually doing while treating patients. The reason for this discrepancy lies in the fact that the therapist is a 'participant and observer' who is called upon constantly to make decisions on the spot. The actual interactional process between therapist and patient is much more complex than the theoretical accounts about it".
On the other hand, given that participants in the Stimulus Group were, in average, younger and with a lesser degree of expertise, might this "generational" and expertise difference explain the intergroup differences? For example, could Actual Neurosis and Anxiety Neurosis be old and "forgotten" or "old-fashioned" concepts to the newer generations of psychoanalysts?
In the case of CBTs, a greater congruence was observed in both studies (i.e., between the Expert Group and the Stimulus Group). However, while expert CBTs stated that GAD was a difficult diagnosis because of its delimitation problems, all the participants who listened to the Stimulus Material preliminarily diagnosed GAD without presenting any difficulties. Also, depression did not appear as a possible comorbid diagnosis in the Stimulus Group of Cognitive-Behavioral therapists, although expert participants highlighted a GAD-depression relationship as a characteristic feature of the disorder. In this sense, the questions presented in the previous paragraph could also apply to the Cognitive-Behavioral participants and thus, extend to the broader scope of subjects related to (a) the insufficiently studied relationship between expertise and case conceptualization47 and (b) the relationship between the theoretical conceptualization or "nomothetic formulation" of clinical problems and the clinical approach in a practice setting, which includes an "idiographic formulation" for a given patient (p. 6)48.
IMPLICATIONS FOR CLINICAL PRACTICE AND RESEARCH
This qualitative research described how Cognitive-Behavioral therapists and Psychoanalysts conceptualize the same notion (Expert Study) and the same patient (Stimulus Study), both regarding Generalized Anxiety Disorder (GAD). In this sense, it may be useful for psychotherapists to develop integrative case formulations and treatment plans by enriching their view of complex realities49, such as the understanding of GAD. In this sense, we hope to contribute to an integrative psychopathological understanding of the study of this diagnosis.
This research may also aid communication among health professionals with differing theoretical orientations which have any kind of joint practice (for example, Psychodynamic psychologists, and Cognitive-Behavioral psychiatrists who provide pharmacotherapy and psychotherapy to the same patient, or those working within the same clinical team), by providing them with GAD's Cognitive Behavioral/Psychoanalytic equivalence language.
We also hope that this study provided material for future practice-informed research about GAD, since clinicians represent an invaluable source of in-situation knowledge that highlights hypotheses to be tested in future research50,51.
LIMITATIONS OF THE STUDY
The present investigation possesses an exploratory nature and thus, its results must only be understood in terms of hypothesis generation. The sampling method used does not estimate its degree of error, hence, the generalizability of the findings obtained is unknown. Likewise, direct conclusions based on differences presented between the Expert Group and the Stimulus Group cannot be drawn because only three expert Ps and one expert CBT participated in the Stimulus Group. Also, since participants in the Stimulus Group were asked to interact with an audio recording of a fictitious patient, interpretations of this study's results in terms of a real life clinical practice should be done with caution. Finally, the results of this paper could either be representing an Argentine phenomenon, or they might be fully or partially generalizable to other cultures.
REFERENCES
1. American Psychiatric Association. "Generalized Anxiety Disorder." Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA. 2013.
2. Roemer, L., Orsillo, S. M., & Barlow, D. H. "Generalized Anxiety Disorder." Anxiety and its disorders.The nature and treatment of anxiety and panic, edited by Barlow. (2nded.). New York: The Guilford Press. 2002/ 2004. pp. 477-515.
3. Etchebarne, I. "Estrategias psicoterapéuticas iniciales para el tratamiento del Trastorno de Ansiedad Generalizada" [Initial Psychotherapeutic Strategies for the Treatment of Generalized Anxiety Disorder]. Doctoral dissertation presented to the Facultad de Psicología. Universidad de Buenos Aires: Buenos Aires. 2014.
4. Freud, S. "Manuscrito B. La etiología de las neurosis". Sigmund Freud. Obras Completas [Sigmund Freud. Complete Works], translated and compiled by J. Strachey. 6tareimpresión. Buenos Aires, Amorrortu Editores, Vol. 1. 1893/1996. pp. 217-223.
5. "Definition of Terms." Diagnostic and Statistical Manual of Mental Disorders. 1st ed. Washington, DC: American Psychiatric Association. 1952, pp. 12-43.
6. "Neuroses." Diagnostic and Statistical Manual of Mental Disorders. 2nd ed. Washington, DC: American Psychiatric Association. 1968, pp. 39-40.
7. "Anxiety Disorders." Diagnostic and Statistical Manual of Mental Disorders. 3rd ed. Washington, DC: American Psychiatric Association. 1980, pp. 225-252.
8. Andrews, G., Hobbs, M. J., Borkovec, T. D., Beesdo, K., Craske, M. G., Heimberg, R. G., Rapee, R. M., Ruscio, A. M., & Stanley, M. A. "Generalized Worry Disorder: A Review of DSM-IV Generalized Anxiety Disorder and Options for DSM-V". Depression and Anxiety, vol. 27, 2010, pp. 134-147.
9. Behar, E., Dobrow DiMarco, I., Hekler, E. B., Mohlman, J., & Staples, A. M. "Current Theoretical Models of Generalized Anxiety Disorder (GAD): Conceptual Review and Treatment Implications". Journal of Anxiety Disorders, vol. 23, 2009, pp. 1011-1023.
10. Newman, M. G., & Llera, S. J. "A novel theory of experiential avoidance in generalized anxiety disorder: A review and synthesis of research supporting a contrast avoidance model of worry". Clinical Psychology Review, vol. 31, 2011, pp. 371-382.
11. Slade, T., & Andrews, G. "DSM-IV and ICD-10 generalized anxiety disorder: discrepant diagnoses and associated disability". Soc Psychiatry Epidemiol, vol. 36, 2001, pp. 45-51.
12. Borkovec, T. D., Alcaine, O. M., y Behar, E. "An Avoidance Theory of Worry and Generalized Anxiety Disorder". Generalized Anxiety Disorder. Advances in Research and Practice [Online versión], compiled by R. G. Heimberg, C. L. Turk, y D. S. Menning. New York: Guilford Press. 2004. http://books.google.com.ar/books?id=klrXMNzWhNMCyprintsec=frontcoveryhl=es#v=onepageyqyf=false
13. Borkovec, T. D., & Inz, J. "The Nature of Worry in Generalized Anxiety Disorder: A Predominance of Thought Activity". Behaviour Research and Therapy, vol. 28, no. 2, 1990, pp. 153-158. Retrieved from http://www.sciencedirect.com/science/article/pii/000579679090027G
14. Newman, M. G., Llera, S. J., Erickson, T. M., Przeworski, A., &Castonguay, L. G. "Worry and Generalized Anxiety Disorder: A Review and Theoretical Synthesis of Evidence on Nature, Etiology, Mechanisms, and Treatment". Annual Review of Clinical Psychology, vol. 9, 2013, pp. 275-297. doi: 10.1146/annurev-clinpsy050212-185544.
15. Llera, S. J., & Newman, M. G. "Rethinking the Role of Worry in Generalized Anxiety Disorder: Evidence Supporting a Model of Emotional Contrast Avoidance." Behavior Therapy. 2014. doi:10.1016/j.beth.2013.12.011
16. Gabbard, G.O. "Psiquiatría psicodinámica en la práctica clínica" [Psychodynamic Psychiatry in Clinical Practice]. 3rd ed.. Buenos Aires: Editorial MédicaPanamericana, S. A. 2000/2002.
17. Gomez-Penedo, J. M. "Conceptualización y abordaje clínico del Trastorno de Ansiedad Generalizada desde la perspectiva del psicoanálisis." [Conceptualization and Clinical Approach to Generalized Anxiety Disorder from a Psychoanalytic Perspective]. Graduate dissertation presented to Facultad de Humanidades, Universidad de Belgrano, Buenos Aires. 2011.
18. Juan, S., Etchebarne, I., Gomez-Penedo, M., & Roussos, A. "Una perspectiva psicoanalítica sobre el Trastorno de Ansiedad Generalizada: Raíces históricas y tendencias actuales." [A Psychoanalytic Perspective on Generalized Anxiety Disorder: Historical Roots and CurrentTrends]. Revista de la Sociedad Argentina de Psicoanálisis, vol. 14, 2010, pp. 197-219.
19. Crits-Christoph, P., Connolly, M.B., Azarian, K., Crits-Christoph, K., & Shappell, S. "An open trial of brief supportive-expressive psychotherapy in the treatment of generalized anxiety disorder." Psychotherapy, vol. 33, no. 3, 1996, pp. 418-430.
20. Crits-Christoph, P., Connolly Gibbons, M.B., Narducci, J., Schamberger, M., & Gallop, R. "Interpersonal problems and the outcome of interpersonally oriented psychodynamic treatment of GAD." Psychotherapy: Theory, Research, Practice, Training, vol .42, no. 2, 2005, pp. 211-224.
21. Ferrero, A., Piero, A., Fassina, S., Massola, T., Lanteri, A., AbbateDaga, G., & Fassino, S. "A 12-month comparison of brief psychodynamic psychotherapy and pharmacotherapy treatment in subjects with generalized anxiety disorders in a community setting." European Psychiatry, vol. 22, 2007, pp. 530-539.
22. Leichsenring, F., Salzer, S., Jaeger, U., Kächele, H., Kreische, R., Leweke, F., Rüger, U., Winkelbach, C., & Leibing, E. "Short-Term Psychodynamic Psychotherapy and Cognitive-Behavioral Therapy in Generalized Anxiety Disorder: A Randomized, Controlled Trial." American Journal of Psychiatry, vol. 166, 2009, pp. 875-881.
23. Crits-Christoph, P. "Psychodynamic-interpersonal treatment of generalized anxiety disorder". Clinical Psychology: Science and practice, vol. 9, no. 1, 2002, pp. 81-84.
24. Borkovec, T. "The nature, functions and origins of worry." In Worrying: Perspectives on theory, assessment and treatment, compliled by G. Davey, & F. Tallis. Sussex, UK: New York Wiley. 1994, pp 5-33.
25. Ferrari, H., Fink, P., Herzig, A., Greenspan, S. I., Hurvich, M. Kaplan, J. A., Kenemore, T. K., Khantzian, E. J., Kirkpatrick, M., Licht, J., Notman, M., & Phillips, D. G. "Symptom Patterns: The Subjective Experience S Axis". In Psychodynamic Diagnostic Manual, compiled by PDM Task Force. Silver Spring, MD: Alliance of Psychoanalytic Organizations. 2006.
26. McWilliams, N., Caligor, E., Herzig, A. Kernberg, O., Shedler, J., &Westen, D. "Personality Patterns and Disorders P Axis". In Psychodynamic Diagnostic Manual, compiled by PDM Task Force. Silver Spring, MD: Alliance of Psychoanalytic Organizations. 2006.
27. McLeod, J. Qualitative Research in Counseling and Psychotherapy. 2nd ed. London: Sage. 2001/2011.
28. Hill, C. "Consensual Qualitative Research [CQR]." Webinar organized by the Society for Psychotherapy Research (November). 2010. Obtained on September 7, 2011 from http://www.psychotherapyresearch.org/displaycommon.cfm?an=1&subarticlenbr=305
29. Hill, C., Knox, S., Thompson, B., Nutt Williams, E., Hess, S., & Ladany, N. "Consensual Qualitative Research: An Uptade." Journal of Counseling Psychology, vol. 52, no. 2, 2005, pp. 196-205.
30. Hill, C., Thompson, B., & Nutt-Williams, E. "A Guide to Conducting Consensual Qualitative Research." The Counseling Psychologist, vol. 25, no. 4, 1997, pp. 517-572.
31. Knox, S., Adrians, N., Everson, E., Hess, S., Hill, C., & Crook-Lyon, R.Clients' Perspectives on Therapy Termination. Psychotherapy Research, vol. 21, no. 2, 2011. pp., 154-167.
32. Eells, T. D., Lombart, K. G., Salsman, N., Kendjelic, E. M., Schneiderman, C. T., & Lucas, C. P. "Expert reasoning in psychotherapy case formulation." Psychotherapy Research, vol. 21 no. 4, 2011, pp. 385-399.
33. Asociación Argentina de Terapia Cognitiva. Certificación. Obtained on September 7, 2011 from http://www.aatc.org.ar/archivos/Certificacion-AATC.pdf
34. Etchebarne, I.; Juan, S.; Balbi, P. & Roussos, A. "El abordaje clínico de la preocupación en el Trastorno de Ansiedad Generalizada: Resultados preliminares" [Clinical Approach to Worry in Generalized Anxiety Disorder: Preliminary Results]. Anuario de Investigaciones, vol. 19, tome I, 2012, pp. 215-223. ISSN 0329-5885, Ediciones de la Facultad de Psicología, Universidad de Buenos Aires.
35. Olivera, J., Braun, M., Gomez-Penedo, J. M., & Roussos, A. "A qualitative investigation of former clients' perception of change, reasons for consultation, therapeutic relationship, and termination." Psychotherapy, vol. 50, no. 4, pp. 505-516.
36. Stiles, W. B. "Logical Operations in Theory-Building Case Studies." [Electronic version]. Pragmatic Case Studies in Psychotherapy, vol. 5, no. 3, 2009, pp. 9-22. Obtained on April 23, 2011 from http://www2.scc.rutgers.edu/journals/index.php/pcsp/article/viewArticle/973
37. Hale, W., Klimstra, T., & Meeus, W. "Is the Generalized Anxiety Disorder Symptom of Worry Just Another Form of Neuroticism? A 5-Year Longitudinal Study of Adolescents From the General Population." Journal of Clinical Psychiatry, vol. 71, no. 7, 2010, pp. 942-948.
38. Vetere, G. Portela, A. & Rodriguez Biglieri, R. "Perfil de personalidad de pacientes con Trastorno de Ansiedad Generalizada." [Personality Profile of Patients with Generalized Anxiety Disorder]. Revista Argentina de Clínica Psicológica, vol. 16, no. 2, 2007, pp. 129-134.
39. Akiskal, H. S. "Anxiety: Definition, Relationship to Depression, and Proposal for an Integrative Model." Anxiety and the Anxiety Disorders, compiled by A. H. Tuma y J. D. Maser. Hillsdale, N J: LEA. 1985, pp. 787-797. Retrieved on 12/10/2012 from http://www.questia.com/read/37096943/anxiety-and-the-anxietydisorders
40. Beck, J. G., Stanley, M. A., & Zebb, B. J. "Characteristics of Generalized Anxiety Disorder in Older Adults: A Descriptive Study." Behaviour Research and Therapy, vol. 34, 1996, pp. 225-234.
41. Etchebarne, I., & Roussos, A. "Modelo de protocolo para presentación de un material estímulo y obtención de datos demográficos de participantes en una investigación." Documento de trabajo # 252, Universidad de Belgrano [Model Protocol for the Presentation of a Stimulus Material and the Recollection of Research Participants' Demographic Data. Working Paper # 252, Universidad de Belgrano]. 2010. Obtained on September 7, 2011 from http://www.ub.edu.ar//investigaciones/dt_nuevos/252_etchebarne.pdf
42. American Psychiatric Association. "El electricista inquieto". DSM-IV. Libro de casos. Compañero del DSM-IV (Manual diagnóstico y estadístico de los trastornos mentales) [DSM-IV. Casebook. DSM-IV (Diagnostic and Statistical Manual and Mental Disorders) Companion] Barcelona: Masson, S. A. 1994/1996.
43. Borkovec, T. D., Robinson, E., Pruzinsky, T., & DePree, J. A. "Preliminary Exploration of Worry: Some Characteristics and Processes." Behaviour Research and Therapy, vol. 21, no. 1, 1983, pp. 9-16. Retrieved from http://www.sciencedirect.com/science/article/pii/0005796783901213
44. Freud, S. "28ª conferencia. La terapia analítica." Sigmund Freud. Obras Completas [Sigmund Freud. Complete Works], compiled and translated by J. Strachey. 6th reprint. Buenos Aires, Amorrortu Editores, vol. 16, 1917/1996, pp. 408-421.
45. Keegan, E. "La ansiedad generalizada como fenómeno: Criterios diagnósticos y concepción psicopatológica [Generalized Anxiety as a phenomenon: Diagnostic Criteria and Psychopathological Conception]." Revista Argentina de Clínica Psicológica, vol. 16, no. 1, 2007, pp. 49-55.
46. Alexander, F. "A Classic in Psychotherapy Integration Revisited: The Dynamics of Psychotherapy in the Light of Learning Theory" [manuscript originally published in 1963]. Journal of Psychotherapy Integration, vol. 14, no. 4, 2004, pp. 347-359. doi:10.1037/1053-0479.14.4.347
47. Eells, T., Lombart, K., "Case formulation and treatment concepts among novice, experienced and experte cognitive-behavioral and psychodynamic therapists." Psychotherapy Research, vol. 13, no. 2, 2003, pp. 187-204.
48. Persons, J. The Case Formulation Approach to Cognitive-Behavior Therapy. New York, Guilford Publications. 2008.
49. Castonguay, L. "Psychotherapy, psychopathology, research and practice: Pathways of connections and integration." Psychotherapy Research, vol. 21, no. 2, 2011, pp. 125-140.
50. Lampropoulos, G. K., Goldfried, M. R., Castonguay, L. G., Lambert, M. J., Stiles, W. B., &Nestoros, J. N. "What Kind of Research Can We Realistically Expect from the Practitioner?" Journal of clinical Psychology, vol. 58, no. 10, 2002, pp. 1241-1264.
51. Polkinghorne, D. "Research and Practitioner Decision Making." Newsletter, 40, Center for KvalitativMetodeudvikling, Department of Psychology, Faculty of Social Sciences, Aarhus University. 2006. Obtained on March 16, 2011 from http://psy.au.dk/en/research/research-centres/center-forkvalitativ-metodeudvikling/newsletter/2006/newsletter-40-june-2006/
1. Doctor in Psychology - (Universidad de Belgrano [UB]) - Benavidez - SP - Argentina
2. Doctor in Psychology - (Universidad de Buenos Aires [UBA])
3. Licensed in Psychology - (Consejo Nacional de Investigaciones Científicas y Técnicas, [CONICET], Universidad de Belgrano [UB], Universidad de Buenos Aires [UBA])
4. Doctor in Psychology - (Consejo Nacional de Investigaciones Científicas y Técnicas, [CONICET], Universidad de Belgrano [UB], Universidad de Buenos Aires [UBA])
Correspondence
Ignacio Etchebarne
Zabala 1837, Ciudad Autónoma de Buenos Aires (C1426DQG)
Buenos Aires, Argentina
igetchebarne@gmail.com
Submitted on: 15/02/2016
Accepted on: 25/07/2016
Institution: Universidad de Belgrano [UB]
* We would like to thank Clara Hill and Bill Stiles for providing us key information (in the form of papers and feedback) that enabled us to conduct this research. We would also like to thank Leonardo Siman for his collaboration with data analysis.
3 Clinical and Theoretical Considerations of Psychoanalysts and Cognitive Behavioral Therapists Regarding Generalized Anxiety Disorder in Argentina. A Qualitative Study of the Research-Practice Gap
APPENDIX A: Interview questions and probes' protocols.
Psychoanalysts' Expert Group protocol:
1. [Grand tour question] Would you please tell me what you think about the DSM's definition of Generalized Anxiety Disorder? [If the participant is unfamiliar with the DSM's criteria, these are read and explained].
2. Do you think GAD is a valid diagnostic category?
3. Within which classical psychoanalytical structure do you consider that GAD is included?
4. What is your position regarding Crits-Christoph's theory of worry in GAD as a defense mechanism?
5. What is your position regarding the PDM's conceptualization of GAD as a Personality Disorder?
6. Do you think GAD is related to the concept of anxiety neurosis?
7. Do you consider GAD is related to the concept of anxiety hysteria?
Cognitive-Behavioral therapists' Expert Group protocol:
1. [Grand tour question] Would you please tell me what you think about the DSM's definition of Generalized Anxiety Disorder?
2. What can you tell me about its proposed definition in the DSM-5, regarding its modifications, such as length and number of worry domains?
3. What do you think about GAD's nature? Is it an anxiety disorder? Is it a personality disorder?
4. What is your position regarding Borkovec's theory of worry in GAD as an avoidance mechanism?
Stimulus Material group protocol
(both Psychoanalysts &Cognitive-Behavioral therapists):
1. [Grand tour probe] Please listen to the following clinical case of 15 minutes in length. This material is a fictional reconstruction of a patient's monologue during a first interview, in which he discusses the problems that brought him to consultation. Please, while you listen to it, imagine that you are the treating therapist and that this is a real patient talking to you, right now, in your office, for his first time. Once the audio recording is over, I'll ask you a few questions.
2. What do you consider to be the patient's main problem?
3. Could you provide a preliminary diagnosis?
APPENDIX B: Examples of Domains, Core Ideas, and Categories (Expert Study).
Domain: GAD's diagnostic validity and delimitation Domain.
Material fragment (Psychoanalyst):
"P: (.) So, DSM's definition doesn't add much for me. When you find yourself with this set of symptoms, that are not a pathology in themselves, you have to make a differential diagnosis among several things."
Core Idea: GAD's diagnostic criteria do not represent a pathology by themselves, with being GAD just a set of symptoms.
Category (Typical): GAD, being a descriptive diagnosis, is insufficient for psychoanalytic conceptualization.
Domain: Functions and/or characteristics of worry in GAD
Material fragment (Cognitive-Behavioral therapist):
"P: Anxiety disorders that aren't GAD are characterized by having a focus of worry, following Barlow's theory about focus. The focus is clear. And actually, GAD has more than one focus or a focus that can easily change. I believe that sometimes GAD's patients don't have many worries at the same time, especially if they are worried about a particular concern, when there is one dominant worry. But they also meet diagnostic criteria. I have a patient whose son has epilepsy, so all day long, she is worrying about that. But if you give her the chance, she would change the theme of the worry. So, the problem is that the therapist may only see one worry in that moment, but if he looks at the patient from a diachronic point of view, he will find different worries."
Core Idea: Although GAD's worry could be focused within a specific area because of the presence of an important problem, it is diachronically perceived as changing through time between different areas.
Category (Variant): Although GAD is characterized by worries that vary across different areas, in some clinical cases, worry could be focused.
APPENDIX C: Examples of Domains, Core Ideas, and Categories (Stimulus Material Study).
Domain: Patient's main problem identified in the Stimulus Material
Material fragment (Cognitive-Behavioral therapist):
"I: From your point of view, what could be the patient's main problem?
P: His main problem is the anxiety activation that produces a high level of uncontrollable worry."
Core Idea: The patient's main problem is the uncontrollable worry.
Category (General): Worry.
Domain: Preliminary diagnosis for the Stimulus Material
Material fragment (Psychoanalyst):
"I: Could you give a preliminary diagnosis for the patient?
P: From a psychoanalytic point of view, it would be an obsessive neurosis. From a DSM point of view, it would be OCD."
Core Idea: From a psychoanalytic perspective, the patient has an obsessive neurosis or, from a DSM point of view, an OCD.
Category (Variant): Obsessive neurosis or DSM-IV-TR's OCD.
APPENDIX D: Team composition, Expectations, & Possible biases.
Team composition:
The team director works as a full time researcher, and he has a Psychodynamic and Integrative clinical background. Two doctors in psychology with part-time dedication to research clinical practice (50% time to each activity) coordinated this project. One of them was a locally certified Cognitive-Behavioral therapist (the first author), and the other was a Psychodynamic therapist (the second author). One doctoral student with a Cognitive-Integrative stance (third author) and one advanced undergraduate psychology student, with a Psychodynamic-Integrative orientation, were also involved in the analysis and write up stages of this study.
Expectations & Possible bias:
In relation to psychoanalysts, we all expected that they would display no familiarity with GAD's diagnosis, that they would disregard it as a descriptive diagnosis, and that they would question its validity. We debated whether they would link GAD either to Anxiety Neurosis, Psychoneuroses, or to primitive anxieties. Also, regarding the patient's main problem in the Stimulus Material, we expected that they would underline the role of anxiety and disregard worryness, since the latter is not conceptualized in clinical psychoanalytic literature. Finally, we all expected GAD to remain as an outsider to psychoanalytic case conceptualizations.
With respect to the Cognitive-Behavioral therapists, we all expected a full acceptance of GAD's diagnosis, as it is presented in the DSM-5 (2013). We also expected them to underline worryness as the main problem in the Stimulus Material, but we could not agree about the degree of acceptance among them, nor could we agree about Borkovec's theory of worry as a cognitive avoidance factor. Likewise, we estimated that they would also present a comorbidity hypothesis regarding the Stimulus Material because of limitations present in the DSM's categorical system.


artigo anterior voltar ao topo próximo artigo