-
Submissão Online Revisar Artigo
Rev. bras. psicoter. 2022; 24(2):43-59
Ferramentas
Artigo Original
Clusters de processamento executivo em crianças com diagnóstico de TDAH
Executive processing clusters in school-age children with ADHD
Clusters de procesamiento ejecutivo en niños diagnosticados con TDAH
Geise Machado Jacobsen, Mirella Liberatore Prando, Gledis Lisiane Correa Luz Motta, Renata Kochhann, Rochele Paz Fonseca
Resumo
Este estudo buscou grupos de processamento executivo em crianças com diagnóstico de Transtorno de Déficit de Atenção/Hiperatividade (TDAH). Para tal, foram utilizadas medidas de flexibilidade cognitiva (FC), inibição (IN) e memória de trabalho (MT) e conduzidas análises de clusters hierárquicos e MANCOVA (p=0.05). Foram identificados três subgrupos com os seguintes perfis de processamento executivo: 1) déficits em FC e IN; 2) déficits em IN; 3) déficits em FC e MT. Esses resultados indicaram a presença de diferentes perfis de déficits em componentes executivos entre crianças com diagnóstico de TDAH. Esses achados podem contribuir para a elaboração de estratégias de intervenção e de programas de psicoeducação para estudantes com diagnóstico de TDAH em contextos clínicos e educacionais.
Descritores: Função Executiva; Transtorno do Deficit de Atenção com Hiperatividade; NeuropsicologiaAbstract
OBJECTIVE: This study aimed to characterize executive processing subgroups among children with Attention Deficit Hyperactivity Disorder (ADHD).
METHOD: Sixty-one children with ADHD, with ages from six to twelve years old, were examined using instruments that evaluate the executive components of cognitive flexibility (CF), inhibition (IN) and working memory (WM). Analysis of hierarchical clusters and MANCOVA (p≤0.05) were conducted.
RESULTS: Participants were divided in three clusters: 1) deficits in CF and in IN; 2) deficits in IN; 3) deficits in CF and in WM.
CONCLUSIONS: the results indicated different neuropsychological profiles among children with ADHD, with different cognitive strengths and weaknesses. Clusters did not differ with respect to biological, clinical, and sociocultural factors. The findings may be useful for educational and health institutions, supporting psychoeducation programs and intervention strategies for students with ADHD.
Keywords: ADHD; ADHD symptoms; Executive functions; Cluster analysis; Neuropsychological functioning
Resumen
Este estudio investigó grupos de procesamiento ejecutivo en niños diagnosticados con trastorno por déficit de atención e hiperactividad (TDAH). Para ello, se utilizaron medidas de flexibilidad cognitiva (FC), inhibición (IN) y memoria de trabajo (MT) y se realizaron análisis de conglomerados jerárquicos y MANCOVA (p=0.05). Se identificaron tres subgrupos con los siguientes perfiles de procesamiento ejecutivo: 1) déficits en FC e IN; 2) déficits en IN; 3) déficits en FC y MT. Estos resultados indicaron la presencia de diferentes perfiles de déficit en los componentes ejecutivos entre los niños diagnosticados con TDAH. Estos datos pueden contribuir al desarrollo de estrategias de intervención y programas de psicoeducación para estudiantes diagnosticados con TDAH en contextos clínicos y educativos.
Descriptores: Función Ejecutiva; Trastorno por Déficit de Atención con Hiperactividad; Neuropsicología
INTRODUCTION
Attention Deficit Hyperactivity Disorder (ADHD) is one of the most common neurodevelopmental conditions in childhood1-3. It is estimated that the prevalence of the condition among children varies from 5% to 7%4-5. The disorder is characterized by persistent symptoms of lack of attention and/or hyperactivity/ impulsivity above what is expected for the age bracket. These symptoms may yield losses in learning, affection, cognition, and social function of children1-3,6-7.
With respect to the neuropsychological profile of ADHD children, individuals with the disorder may present deficits in multiple neurocognitive processes and related cerebral systems. Also, different people can indicate different neuropsychological profiles, which only add to the complex and heterogenic characteristics of the condition8-9. Despite the diversity in cognitive profiles, deficits in executive functions (EF) components have been pointed as some of the main characteristics of ADHD10-12. Executive functions are a group of cognitive processes that work together to produce, execute, monitor, regulate, and readjust adequate conducts to attain complex goals13. According to Diamond14, these abilities can be comprehended through a model that includes the main components of cognitive flexibility, inhibition, and working memory, as well as the complex components of reasoning and problem solving.
In this sense, symptoms related to the disorder would arise from primary losses in executive components, such as inhibition or working memory, or even general executive difficulties. This proposal is based on evidence that pre-frontal lesions can produce symptoms associated with ADHD1,12,15-16. Barkley17, for example, proposes that the main ADHD characteristic is an inhibition deficit that harms other aspects of executive functioning.
According to Barkley17, inattention refers to the incapacity of maintaining attention on activities or tasks, remembering and following instructions or rules, and avoiding distractions. The author believes that ADHD's distinct inattention can be a consequence of executive problems, especially of working memory. On the same note, impulsivity is related to inhibition difficulties, involving losses in the ability to inhibit responses.
Overall, studies have found deficits in executive components such as cognitive flexibility, verbal fluency, inhibition, working memory, planning and vigilance, as well as difficulties in sustained attention3,12,16,18-19. Even though EF component deficits are prevalent in ADHD, they may not be present in all individuals who have the disorder10. Also, they are not specific to this condition and they are not necessary to reach diagnosis3.
Some studies have not detected differences between executive functions among the various presentations of ADHD20-21. Even so, there is evidence to support a distinct neuropsychological profile between presentations. Problems with learning and language (loss in comprehension, mathematics, and writing, for example) are more frequently associated with the predominantly inattentive type3,21-22. Executive deficits, on the other hand, are more closely related to the combined and hyperactive-impulsive types6,21. In summary, attention problems can generate more academic losses, while hyperactivity-impulsivity problems are more closely linked to behavioral issues. Working memory deficits are also associated with attention problems23.
Considering the neuropsychological profile heterogeneity among children with ADHD, especially with respect to EF, it is necessary to invest in understanding some key factors. Those include the specific aspects of executive components processing within the disorder, as well as which biological, individual, sociocultural, and clinical factors may explain the variability of the executive profiles. In order to investigate the executive abilities of abilities of children with ADHD, along with the variables that may be associated with their differences, cluster analyses may be performed.
However, studies about ADHD that have used this method are scarce. The majority of them have approached the differences between symptoms of inattentiveness and hyperactivity24-26 inattention, hyperactivity, and impulsivity, are expressed with various degrees of severity. The nature of the biological dysfunction sustaining each subtype (common or distinct. Only three researches have investigated differences in cognitive profiles between clusters. Bonafina, Newcorn, McKay, Koda and Halperin27 have analyzed subgroups of intellectual and reading abilities. Thaler and collaborators7 investigated subgroups of cognitive abilities in a sample of children with predominantly inattentive or combined ADHD types, based on WISC-IV. The first cluster presented reduced processing speed and higher incidence of diagnosis for the predominantly inattentive type, whereas the second cluster showed deficits in processing speed and working memory, as well as predominance of behavioral problems. Only one research has approached FE and ADHD clusters more specifically28. Three clusters were found: 1) difficulties in inhibitory control, 2) cognitive flexibility and processing speed problems, and 3) a subgroup with no executive losses. However, this investigation used only two EF measures: Stop Task, to evaluate inhibition, and Trail Making Task, to measure cognitive flexibility and processing speed. Therefore, studies that approach other EF evaluation paradigms are necessary, and they should include verbal measures as well as working memory examinations. That would allow the investigation of specific aspects of the different executive components and task models. Moreover, biological and sociocultural factors, as well as the intensity of inattention and hyperactivity symptoms, are yet to be studied and analyzed with respect to their impact on executive deficits that may be present in ADHD. In this context, the present study aimed 1) to identify subgroups within a sample of children with ADHD regarding the processing profile of the following executive components: cognitive flexibility, inhibition, and working memory; and 2) to identify whether clusters present differences concerning biological, clinical, and sociocultural factors.
METHOD
Procedures
The children were referred to participate in the research by two sources in Porto Alegre, Brazil: the Child Psychiatric Ambulatory team from a hospital, and health professionals from the private sector. Contact was made with parents and/or guardians to invite them to participate in the research. After the explanation of the study's goals, as well as details about ethical and data collection procedures, parents and/or guardians signed an informed consent form.
Participants were evaluated in a school clinic or in a private clinic in Porto Alegre. The children were individually assessed in two sessions that lasted around one hour each. With permission from the physician in charge, children who were under psychostimulant medication for ADHD had treatment suspended for a period of 24 or 48 hours before their assessment, depending on the type of medication.
Participants
Sixty-one children participated in this study. Selected individuals were between 6 and 12 years old (mean 9.18; standard deviation 1.56), from both genders (feminine: n=20; masculine: n=41), and enrolled in private (n=42) or public (n=19) schools. The following criteria were considered for exclusion: a) uncorrected sensory impairments (auditory and/or visual); b) history of neurological conditions; c) history of primary psychiatric disorders regarding ADHD; d) intelligence quotient (IQ) lower than 80, according to Wechsler Abbreviated Scale of Intelligence (WASI) (29); and e) participation in neuropsychological rehabilitation for EFs. From the initial sample of 80 participants, n=4 were excluded because they did not fulfill ADHD diagnostic criteria; n=13 were excluded because they presented IQ lower than 80, according to WASI; and n=2 were excluded due to history of neurological condition. Hence, there was a total of 19 exclusions.
Participants were diagnosed with ADHD by a neurologist or a psychiatrist from the referral sources. The diagnosis was confirmed by the researchers through a semi-structured clinical interview (Kiddie-Sads; 30) with the child and his/her parents and/or guardians, and complemented by data from the MTA-SNAP-IV questionnaire (31), filled by parents and/or guardians and by teachers of the participant. Children had either the inattentive (n=30) or the combined (n=31) presentation of ADHD. In the assessment made through the MTA-SNAP-IV questionnaire, on average, participants showed 6.36 (SD=1.47) inattentive symptoms with mean intensity of 16.11 (SD=3.86), and 4.16 (SD=2.81) hyperactivity symptoms with mean intensity of 11.83 (SD=6.21).
Among the 61 participants, n=43 showed writing and reading deficits in tasks of reading words and pseudowords to examine reading routes, and of writing under dictation to assess orthographic processing. Those tasks were used to track difficulties in these processes, due to the high level of comorbidity with learning disorders. Also, n=7 children presented comorbidity with other psychiatric disorders, being n=2 of them with diagnosis of anxiety; n=2 with depression; n=1 with bipolar disorder; n=1 with oppositional defiant disorder; and n=1 with enuresis. Comorbidities were informed by the neurologist or by the psychiatrist in charge of assisting the participant.
Instruments
1) Unconstrained Verbal Fluency (UVF), adapted for children by Jacobsen and collaborators (32) from the Montreal Communication Evaluation Battery33-34. Verbal fluency tasks assess executive and lexical-semantic processes, demanding attention, information update, capacity to: start the search, retrieve information from the lexicon, and organize a search strategy. They also require cognitive flexibility, inhibition, and working memory. During the UFV task, without phonemic-orthographic or semantic criteria, the child must recall as many words as possible during two minutes and thirty seconds, except for proper nouns (cities, countries, people, etc.) and numbers. Total switches (shifts between categories) are taken into consideration during task execution.
2) Narrative Discourse (ND), adapted for children by Prando and collaborators (35) from the Montreal Communication Evaluation Battery33-34. The instrument evaluates complex linguistic processing, as well as episodic and working memory. The task involves three steps: 1) partial retelling, in which the examiner reads a brief story, paragraph by paragraph, and, after each one, the child must retell it; 2) integral retelling, in which the examiner retells the complete story and, right after that, the participant must tell it with his/her own words; 3) text comprehension, in which the child is asked 11 questions about the story. The score of essential information retrieved during partial retelling (main elements of the story) is included in this study.
3) Wechsler Intelligence Scale for Children 3rd edition (WISC-III)36. Battery that allows the characterization of the neuropsychological profile from the assessment of various cognitive functions. The Digits subtest was applied, allowing the examination of selective auditory attention (direct order - DO) and of central executive system of working memory (inverse order - IO). In DO, the participant must repeat a sequence of numbers in the same order that he/she heard them. In IO, on the other hand, the participant must repeat them backwards. This study uses the following measures: total of correct responses in IO and discrepancy between the two parts of the test, which corresponds to the OD raw score minus the OI raw score.
4) Hayling Sentence Completion Test for Children (HSCT-C), adapted for Brazilian children by Siqueira and collaborators37, from the original version by Burgess and Shallice38. Task composed of two parts in which the participant must complete sentences whose last word is missing. Both parts of the instrument assess attention and processing speed. In the transition between parts A and B, cognitive flexibility ability may be observed. Specifically, part A is more closely related to the examination of verbal initiation and lexical search, whereas part B is more associated with the measurement of verbal inhibition and planning. In part A, the child must evoke, as quickly as possible, a word that coherently completes each of the ten sentences. Semantic and syntactic context leads to the activation of a coherent vocabulary. In part B, the examinee must complete the sentence with a word that is not related to the semantic and syntactic context, that is, he/she must inhibit the dominant word. This study includes scores for execution time (latency to respond to sentences), total number of mistakes in part B (words that have semantic association with the sentence), and execution time in part B minus execution time in part A.
Data analysis
Data were analyzed using SPSS 17.0 software for Windows, with a significance level of p≤0.05. Scores from tasks that assess the executive components of cognitive flexibility, inhibition, and central executive system of working memory were converted into Z scores, considering normative data from each instrument. From the Z scores, an EF general compound score, as well as a specific compound score for each executive component, was calculated, as shown in Figure 1. The general compound score includes all scores provided by each executive component. A hierarchical cluster analysis was conducted, using EF general compound score as the classification criterion. Given that three executive components were examined and that Roberts and collaborators (28) identified three groups in their study, three clusters were requested. Differences among clusters with respect to the following nominal variables were verified through a Chi-Square test: presentation of the disorder (combined or inattentive), difficulties in reading and writing (absence or presence), parental level of education (high or low), occurrence of deficits (absence or presence), gender (feminine or masculine), and type of school (private or public). Differences regarding age were examined using One-Way ANOVA. Because differences in age were coterminous and associations between different scores could occur, MANCOVA was conducted. In that analysis, age was controlled in order to verify differences between clusters with respect to compound scores, raw scores from EF tasks, and frequency/intensity of ADHD symptoms measured by MTA-SNAP-IV questionnaire.

Figure 1. Score composition of cognitive flexibility, inhibition, and working memory
RESULTS
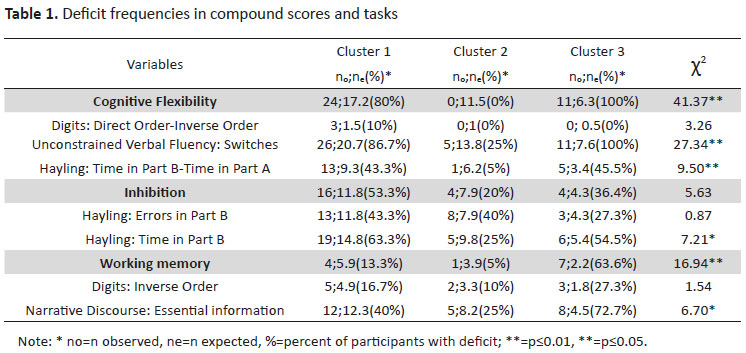
Considering the EF general compound score, participants were distributed in three executive performance clusters (cluster 1: n=30; cluster 2: n=20; cluster 3: n=11). Table 1 describes the deficit frequencies of each cluster in compound scores and in neuropsychological tasks. Cluster 1 presented high prevalence of deficits in cognitive flexibility and inhibition. Cluster 2 showed low prevalence of losses, but deficits in inhibition were observed. Finally, cluster 3 evidenced 100% loss in cognitive flexibility, high prevalence of deficits in working memory, and losses in inhibition. Differences were significant in compound scores of cognitive flexibility and working memory. There were no significant differences in inhibition scores.

Regarding neuropsychological tasks, there was low prevalence of deficits in the discrepancy score from the Digits subtest in all three clusters, with no significant differences. On the subject of UVF total switches, there was high prevalence of deficits in clusters 1 and 3, wherein cluster 3 there was 100% loss. Similarly, discrepancies in HSCT-C times presented high prevalence of deficits in clusters 1 and 3. Regarding total number of errors in part B of HSCT-C, there was relatively high prevalence of deficits, especially in clusters 1 and 2, but differences were not significant. In execution time of HSCT-C, there was significant prevalence of losses in cluster 1. There was no significant prevalence of deficits in Digits IO score. Finally, ND showed higher prevalence of deficits in cluster 3.
Table 2 displays MANCOVA results, with controlled age, comparing cognitive profile of clusters in compound scores. In order to ensure clear results, this table also shows means and standard deviations for Z scores in participants' compound scores and in tasks. In cognitive flexibility score, there were significant differences among all groups, being cluster 3 the most hindered, followed by cluster 1. In inhibition score, cluster 1 had the most deficit and was significantly different from cluster 2, which was the most preserved. In working memory score, clusters 1 and 2 showed homogenous performance, whereas cluster 3 was the most impaired.

Table 3 shows MANCOVA results that compared cluster performance results with regards to raw scores from neuropsychological tasks. Total UVF switches demonstrated differences in all groups, being cluster 3 the most hindered, followed by cluster 1. Regarding time in part B of HSCT-C, cluster 1, with the most performance deficit, differed from cluster 3, the most preserved. In ND, there were significant differences between clusters 3 and 2, being cluster 3 the most hindered and cluster 2 the most preserved.

Regarding age, inattentive and hyperactivity/impulsivity symptoms, intelligence quotient, occurrence of ADHD, difficulties in reading and writing, parental level of education, gender, and type of school, there were no significant differences. Differences with respect to age were coterminous (p=0.06), being cluster 3 the oldest.
DISCUSSION
This study aimed to identify executive function subgroups in a sample of children diagnosed with ADHD and characterize possible differences regarding biological, clinical, and sociocultural factors. Three clusters were identified: 1) high frequency and gravity of losses in cognitive flexibility and inhibition; 2) more preserved, with low frequency of deficits and slight losses in inhibition; and 3) high frequency and gravity of deficits in cognitive flexibility and working memory and, in smaller proportion, also inhibition. These results are similar to those of Roberts and collaborators28, who have also detected a subgroup with losses in cognitive flexibility and another with deficits in inhibition. However, these authors identified a preserved subgroup, probably due to the assessment with visuospatial paradigms. The present study, however, contributes with another perspective on processing these components in children with ADHD, since it utilized verbal modalities for evaluating cognitive flexibility and inhibition, whereas Roberts and collaborators28 focused on visuospatial instruments. Furthermore, this research assessed the component of central executive system of working memory, which was not operationalized in the neuropsychological evaluation paradigms selected in the study by Roberts and collaborators28. Finally, in this study, clusters were compared considering Z scores and frequency of deficit occurrence, which allow a more clinical assessment of dissociations when compared to the investigation performed by Roberts and collaborators28.
All three clusters presented losses in inhibition, especially cluster 1. That may suggest that there is possibly a slight base inhibitory loss in this sample. In part, this finding is in accordance with the hybrid model proposed by Barkley17 to understand ADHD. Barkley17 proposed that this clinical condition was characterized by a deficit in behavior inhibition, which would generate losses in functioning of other related executive components. More specifically, behavioral inhibition, which involves control over automatic/dominant responses and interference, as well as current response interruption, would contribute to the performance in other executive components: 1) working memory (keep in mind and manipulate events and information); 2) autoregulation of affection, motivation, and alertness (self-control of emotions and autoregulation of alertness and motivation in favor of attaining objects); 3) discourse internalization (description and reflection, problem solving, moral reasoning); and 4) reconstitution (synthesis and analysis of behaviors, behavioral and verbal fluency, behavioral creativity directed to objectives). Therefore, because of its role in processing these components, primary loss in inhibition would generate or leverage deficits in self-control and behaviors directed to objectives. Indirectly, it also harms the control over motor responses oriented towards objectives, also being influenced by the four components of the model. Thus, differently from individuals in general, who guide their behaviors based on internal representations, people with ADHD base their behavior more heavily on the immediate context and on direct consequences.
With that said, results from the present study are similar to Barkley's proposal17 because they indicate a trend towards a general loss in the inhibition component of all three clusters, even though it is through the lens of attention and cognitive inhibition rather than behavioral. It is suggested that slight base deficits or the comorbidity with inhibition losses may leverage deficits in other executive components. However, in this sample, not all participants presented deficits in inhibition measurements, and not all executive components were affected, as suggested by the model. Theories to understand ADHD have evolved since Barkley's proposal17. In addition, it is agreed that not all individuals diagnosed with ADHD present executive deficits, even though those are highly prevalent. It is also a consensus that there may exist different neuropsychological profiles, with various cognitive components affected3,9,12,15. On the other hand, the hypothesis that losses in inhibition control would be one of the main characteristics of ADHD has been supported by literature16,20,39-40 substantial evidence supporting heterogeneity in neuropsychological performance among youth with ADHD as well as apparent effect differences by sex, age, and comorbidity have slowed progress. To address this, it is important to understand sibling effects in relation to these moderators. 461 youth ages 6-17 years (54.8\u00a0% male, including 251 youth with ADHD, 107 of their unaffected biological siblings, and 103 non-ADHD controls.
Cognitive flexibility was the component that presented the most losses in frequency and gravity in clusters 1 and 3. Cluster 3 also displayed high prevalence and gravity of deficits in working memory. Clusters 1 and 3 also showed highest prevalence of losses in inhibition. Hence, it is suggested that base deficits in inhibition may contribute to losses in cognitive flexibility and working memory, as observed in this sample, and as predicted under Barkley's model17. It is known that the ability to use inhibition evidences interrelations with abilities of cognitive flexibility and working memory41-42. For example, to attain a goal, it is necessary to keep relevant information in mind in order to determine which affections, behaviors and/or thoughts are appropriate to inhibit. In the same sense, it is necessary to inhibit distracting stimuli, irrelevant information, and internal predispositions, with the purpose of manipulating multiple facts or ideas and being flexible to adapt to demands from the context or task14.
Regarding specific results for each task, under the component of flexibility, scores for switches under the UVF task and for discrepancy of HSCT-C execution times were differentiators for the groups. Clusters 1 and 3 showed high frequency and gravity of deficits in these measures, especially in the number of switches. In the inhibition component, execution time for part B of HSCT-C differentiated the groups, being cluster 1 the most hindered, followed by cluster 3. Finally, in the working memory component, ND differentiated the groups, being cluster 3 the one with the most deficit. The tasks that differentiated the groups and that presented more prevalence and gravity of deficits either assess the speed to inhibit an automatic/dominant response, or are mediated by language (such as switches in UVF and ND tasks). In this sample, participants displayed a tendency to be able to inhibit the preponderant response, but they took longer than expected to do it (HSCT-C Time B). Cognitive flexibility deficits may be related to a slow processing time to adapt to new demands and tasks (HSCT-C TB-TA). They may also be related to a loss in lexical-semantic processing, which appears through difficulties in manipulating verbal categories (UVF switches). Working memory deficits also became more evident in tasks that demand the manipulation of verbal information (ND). That suggests, once again, the cooperation between cognitive flexibility and working memory, especially when linguistic complexity is involved, in a discourse level of language. Therefore, children from this sample seem to present more difficulty in evoking, processing, and manipulating verbal information. Participants demonstrated high prevalence of deficits in reading and writing, but with no significant differences.
In summary, the three executive components evaluated were important to understand the neurocognitive profile of the sample, since each cluster has presented distinct profiles of abilities that showed losses and that were preserved. Findings of this study contribute with more evidence that there is no single neuropsychological profile in ADHD cases. Different individuals may present different patterns of executive processing, with distinctive cognitive strengths and weaknesses. With that said, models for understanding ADHD such as Barkley's17 and Rapport's43, which define, respectively, inhibition and working memory deficits as main characteristics of the disorder, seem not to include the complexity of the condition's neuropsychological profiles. In this sample, even though deficits in inhibition and working memory were essential to characterize the clusters, not all participants presented deficits in these components, and there were distinct profiles among the groups. In fact, the component of cognitive flexibility showed the most prevalence and gravity of deficits and the most sensibility to distinguish groups, differentiating the three clusters.
Even though studies have reported losses in cognitive flexibility16,44-45, investigations about the neuropsychological profile of children with ADHD tend to emphasize the pattern of deficits in inhibition and working memory. Therefore, the present findings contribute with evidence about the importance of assessing cognitive flexibility abilities to characterize and understand the cognitive profile of children with ADHD. This was the most frequent and severely affected component in this sample. Results of this study are also in accordance with the pattern of losses in inhibition45-46 and working memory47-48 described in the literature. Although, in this sample, processing of inhibition, working memory, and cognitive flexibility became more complex when mediated by language and processing speed, probably due to high frequency of losses in reading and writing.
With regards to biological, clinical, and sociocultural factors, there were coterminous differences in age, being cluster 3 the most hindered and the oldest, which may be associated with the course of the disorder. The following variables did not present significant differences between clusters: gender, presentation of the disorder (predominantly inattentive or combined types), frequency/intensity of symptoms of inattentiveness and hyperactivity/impulsivity, presence of difficulties in reading and writing, type of school, and parental level of education. In this sample, the expression of the clinical condition overcomes even factors that, according to the literature, could be protective for executive processing, such as parents with high level of education and attending private school. Families with higher education and whose children attend private school, according to studies, tend to offer more opportunities of cognitive stimulation, which could favor the executive development49-51. Socioeconomic variables may be more closely associated with the increased risk of developing the disorder than with the profile and the gravity of cognitive deficits52-53 the United States and Australia have found an association between childhood attention deficit hyperactivity disorder (ADHD. Lack of differences in gender may indicate that, even though prevalence of ADHD is higher among boys, the disorder may manifest itself similarly in both genders54.
Results concerning clinical characteristics are in agreement with literature. Geurts e colaboradores6 have not identified differences in executive profile between predominantly inattentive and combined types for the following measurements: cognitive flexibility, verbal fluency, inhibition, working memory, and planning. Willcutt5 mentions that there are few evidences about the differences in neurocognitive profile between these types. The same author, when referring to the previous classification of DSM-IV, says that there was not much validity in classifying subtypes due to the lack of evidence regarding distinguishing validity between predominantly inattentive and combined types, and longitudinal stability of the three subtypes. Because of changes in predominant symptoms through the course of the disorder, in DSM-5, the subtypes started being regarded as presentations, but are still classified and distinct profiles.
With regards to frequency/intensity of symptoms, Jonsdottir e colaboradores3 have not found significant relationship between testimonials of parents and teachers about the ADHD symptoms, and the child's performance in tasks involving selective and sustained attention, verbal working memory, and planning. Coghill, Hayward, Rhodes, Grimmer and Matthews55, similarly, have not identified a relationship between changes in ADHD symptoms and variations in executive performance measured by cognitive flexibility and planning tasks. The authors say that the hypothesis of a linear relationship between symptoms and cognitive deficits is too simplistic. So, they suggest that the symptoms not necessarily arise as a consequence of cognitive losses. Cognitive deficits, in turn, may not be related to central symptoms of the disorder and generate compromises independently of them. Therefore, in contrast with the traditional model, the increment in cognitive processing may not result in improvement of symptoms, but it may contribute to an improvement in the individual's functionality. Finally, concerning difficulties in reading and writing, significant differences may not have been found due to high prevalence of losses in these abilities in all three clusters (these are some of the main comorbidities of ADHD)1,56, and due to the assessment through words.
Future studies must advance with respect to the comparison between visuospatial and verbal modalities when assessing executive functions, since this study used mainly verbal measurements, while Roberts and collaborators28 used mostly visuospatial ones. The results of this study are not to be generalized, since the sample is not representative of the population of children diagnosed with ADHD. Nevertheless, this is the first study that evaluates executive profiles of Brazilian children diagnosed with ADHD through cluster analysis, and through research about biological, clinical, and sociocultural factors particular to countries under development. Findings from this study contribute with evidence about diversity of executive profiles within the disorder, highlighting the importance of cognitive flexibility when characterizing the condition. Another important point is the role of language and of processing speed as possible mediators of deficits in other executive components. From the results on dissociations of executive abilities in ADHD, a contribution in planning the assessment and rehabilitation of executive deficits becomes possible. Findings from this study may also be useful for education and health institutions, by serving as a base to promote programs of psychoeducation to care givers and educators. Also, it may contribute to build intervention strategies within executive functions in the context of clinical and pedagogical practices.
REFERENCES
1. Brocki K, Bohlin, G (2006) Developmental change in the relation between executive functions and symptoms of ADHD and co-occurring behaviour problems. Infant and Child Development, 15(1), 19-40. doi:10.1002/ icd.413
2. Costa D, Paula J, Alvim-Soares Júnior A, Diniz B, Romano-Silva M, Malloy-Diniz L, Miranda D (2014) ADHD inattentive symptoms mediate the relationship between intelligence and academic performance in children aged 6-14. Braz J Psychiatry 00(ahead): 000-000. doi:10.1590/1516-4446-2013-1201
3. Jonsdottir S, Bouma A, Sergeant J, Scherder E (2006) Relationships between neuropsychological measures of executive function and behavioral measures of ADHD symptoms and comorbid behavior. Arch Clin Neuropsychol 21: 383-94. doi:10.1016/j.acn.2006.05.003
4. Polanczyk G, de Lima M, Horta B, Biederman J, Rohde L (2007) The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry 164: 942-8. doi:10.1176/appi.ajp.164.6.942
5 . Willcutt E (2012) The prevalence of DSM-IV attention-deficit/hyperactivity disorder: a meta-analytic review. Neurotherapeutics 9: 490-9. doi:10.1007/s13311-012-0135-8
6. Geurts H, Verté S, Oosterlaan J, Roeyers H, Sergeant J (2005) ADHD subtypes: do they differ in their executive functioning profile? Arch Clin Neuropsychol 20: 457-77. doi:10.1016/j.acn.2004.11.001
7. Thaler N, Bello D, Etcoff L (2012) WISC-IV profiles are associated with differences in symptomatology and outcome in children with ADHD. J Atten Disord 17: 291-301. doi:10.1177/1087054711428806
8. Gonzalez-Gadea M, Baez S, Torralva T, Castellanos F, Rattazzi A, Bein V, et al. (2013) Cognitive variability in adults with ADHD and AS: disentangling the roles of executive functions and social cognition. Res Dev Disabil 34: 817-830. doi:10.1016/j.ridd.2012.11.009
9. Sonuga-Barke E, Coghill D (2014) Editorial perspective: laying the foundations for next generation models of ADHD neuropsychology. J Child Psychol Psychiatry 55: 1215-7. doi:10.1111/jcpp.12341
10. Kofler M, Irwin L, Soto E, Groves N, Harmon S, Sarver D (2018) Executive functioning heterogeneity in pediatric ADHD. J Abnorm Child Psychol. doi: https://doi.org/10.1007/s10802-018-0438-2
11. Dovis, S., Maric, M., Prins, P., & Van der Oord, S. (2019). Does executive function capacity moderate the outcome of executive function training in children with ADHD? ADHD Attention Deficit and Hyperactivity Disorders. doi: https://doi.org/10.1007/s12402-019-00308-5
12. Willcutt E, Doyle A, Nigg J, Faraone S, Pennington B (2005) Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review. Biol Psychiatry 57: 1336-46. doi:10.1016/j. biopsych.2005.02.006.
13. Verdejo-García A, Bechara A (2010) Neuropsicología de las funciones ejecutivas. Psicothema 22: 227-235. Retrieved from: http://www.redalyc.org/articulo.oa?id=72712496009.
14. Diamond A (2013) Executive functions. Annu Rev Psychol 64: 135-68. doi:10.1146/annurevpsych-113011-143750
15. Doyle A, Faraone S, Seidman L, Willcutt E, Nigg J, Waldman I, et al. (2005) Are endophenotypes based on measures of executive functions useful for molecular genetic studies of ADHD? J Child Psychol Psychiatry 46: 774-803. doi:10.1111/j.1469-7610.2005.01476.x
16. Holmes J., Gathercole, S., Place, M., Alloway, T., Elliott, J., & Hilton, K. (2010). The diagnostic utility of executive function assessments in the identification of ADHD in children. Child and Adolescent Mental Health, 15(1), 37-43. doi:10.1111/j.1475-3588.2009.00536.x
17. Barkley R A (1997) Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD. Psychol Bull 121: 65-94. Retrieved from: https://pdfs.semanticscholar.org/79fc/ a744b773204851ac94f0aaaaa03b7d799d80.pdf
18. Fischer M, Barkley R, Fletcher K, Smallish L (2005) Executive functioning in hyperactive children as young adults: attention, inhibition, response perseveration, and the impact of comorbidity. Dev Neuropsychol 27: 107-33. doi:10.1207/s15326942dn2701_5
19. Semrud-Clikeman M, Walkowiak J, Wilkinson A, Butcher B (2010) Executive functioning in children with Asperger syndrome, ADHD-combined type, ADHD-predominately inattentive type, and controls. J Autism Dev Disord 40: 1017-27. doi:10.1007/s10803-010-0951-9
20. Geurts H, Verté S, Oosterlaan J, Roeyers H, Sergeant J (2004) How specific are executive functioning deficits in attention deficit hyperactivity disorder and autism? J Child Psychol Psychiatry 45: 836-54. doi:10.1111/ j.1469-7610.2004.00276.x
21. Riccio C, Homack S, Jarratt K, Wolfe M (2006) Differences in academic and executive function domains among children with ADHD Predominantly Inattentive and Combined Types. Arch Clin Neuropsychol 21: 657-67. doi:10.1016/j.acn.2006.05.010
22. Bellani M, Perlini C, Brambilla P (2011) Language disturbances in schizophrenia. Epidemiol Psychiatr Sci 18: 314-317. doi:10.1017/S2045796011000527
23. Bunford N, Brandt N, Golden C, Dykstra J, Suhr J, Owens J (2014) Attention-Deficit/Hyperactivity Disorder symptoms mediate the association between deficits in executive functioning and social impairment in children. J Abnorm Child Psychol. doi:10.1007/s10802-014-9902-9
24. Blondeau C, Dellu-Hagedorn F (2007) Dimensional analysis of ADHD subtypes in rats. Biol Psychiatry 61: 1340-50. doi:10.1016/j.biopsych.2006.06.030
25. Elia J, Arcos-Burgos M, Bolton K, Ambrosini P, Berrettini W, Muenke M (2009) ADHD latent class clusters: DSM-IV subtypes and comorbidity. Psychiatry Res 170: 192-8. doi:10.1016/j.psychres.2008.10.008
26. Marsh, P., & Williams, L. (2004). An investigation of individual typologies of attention-deficit hyperactivity disorder using cluster analysis of DSM-IV criteria. Personality and Individual Differences, 36(5), 1187-1195. doi:10.1016/S0191-8869(03)00210-1
27. Bonafina M, Newcorn J, McKay K, Koda V, Halperin J (2000) ADHD and reading disabilities a cluster analytic approach for distinguishing subgroups. J Learn Disabil 33: 297-307. Retrieved from: http://ldx.sagepub. com/content/33/3/297.long
28. Roberts B, Martel, M, Nigg J (2013) Are there executive dysfunction subtypes within ADHD? J Atten Disord. doi:10.1177/1087054713510349
29. Trentini C, Yates D, Heck V (2014) Escala Wechsler Abreviada de Inteligência [Weschler Abbreviated Scale of Intelligence]. Pearson.
30. Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, et al. (1997) Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry 36: 980-988. Retrieved from: http://www.sciencedirect. com/science/article/pii/S0890856709625557
31. Mattos P, Serra-Pinheiro M, Rohde L, Pinto D (2006) A Brazilian version of the MTA-SNAP-IV for evaluation of symptoms of attention-deficit/hyperactivity disorder and oppositional-defiant disorder. Trends Psychiatry Psychother 28: 290-297. Retrieved from http://www.scielo.br/scielo.php?script=sci_arttext&pid=S010181082006000300008&lng=en&tlng=pt.
32. Jacobsen G, Prando M, Moraes A, Pureza J, Gonçalves H, Siqueira L, et al. (2016) Effects of age and school type on unsconstrained, phonemic and semantic verbal fluency in children. Appl Neuropsychol Child 0: 1-14. doi: 10.1080/21622965.2015.1072535
33. Fonseca R, Parente M, Côté H, Ska B, Joanette Y (2008) Bateria Montreal de Avaliação da Comunicação [Montreal Communication Evaluation Battery]. Pró-Fono.
34. Joanette Y, Ska B, Côté H (2004) Protocole Montréal d'Évaluation de la Communication [Montreal Communication Evaluation Battery]. Ortho.
35. Prando M, Jacobsen G, Gonçalves H, Siqueira L, Moraes A, Pureza J, et al. (2016) Discurso Narrativo Oral Infantil [Child Oral Narrative Discourse]. In: Tarefas para avaliação neuropsicológica [Tasks for neuropsychological evaluation]. Memnon.
36. Figueiredo V (2002) Escala de Inteligência Wechsler para Crianças [Wechsler Intelligence Scale for Children]. Casa do Psicólogo.
37. Siqueira L, Gonçalves H, Pagliarin K, Prando M, Jacobsen G, Pureza J, et al. (2016) Teste Hayling Infantil [Child Hayling Test]. In: Tarefas para avaliação neuropsicológica [Tasks for neuropsychological evaluation]. Memnon.
38. Burgess P, Shallice T (1997) The Hayling and Brixton tests. Thames Valley Test Company.
39. Gau S, Shang C-Y (2010) Executive functions as endophenotypes in ADHD: evidence from the Cambridge Neuropsychological Test Battery (CANTAB). J Child Psychol Psychiatry 51: 838-49. doi:10.1111/j.14697610.2010.02215.x
40. Nikolas M, Nigg J (2014) Moderators of neuropsychological nechanism in Attention-Deficit Hyperactivity Disorder. J Abnorm Child Psychol 271-281. doi:10.1007/s10802-014-9904-7
41. Dovis S, Van der Oord S, Huizinga H, Wiers R, Prins P (2014) Prevalence and diagnostic validity of motivational impairments and deficits in visuospatial short-term memory and working memory in ADHD subtypes. Eur Child Adolesc Psychiatry 1-16. doi: 10.1007/s00787-014-0612-1.
42. Pureza J, Jacobsen G, Oliveira R, Fonseca R (2011) Relationships between executive functions tasks in late childhood. Psychology & Neuroscience, 4(3), 369. doi: 10.3922/j.psns.2011.3.010
43. Rapport L, Van Voorhis A, Tzelepis A, Friedman S (2001) Executive functioning in adult attention-deficit hyperactivity disorder. Clin Neuropsychol 15: 479-491. Retrieved from: http://www.tandfonline.com/doi/ abs/10.1076/clin.15.4.479.1878#.VosNUBUrLIU
44. Marzocchi G, Oosterlaan J, Zuddas A, Cavolina P, Geurts H, Redigolo D, et al (2008) Contrasting deficits on executive functions between ADHD and reading disabled children. J Child Psychol Psychiatry 49: 543-52. doi:10.1111/j.1469-7610.2007.01859.x
45. Sjöwall D, Roth L, Lindqvist S, Thorell L (2013) Multiple deficits in ADHD: executive dysfunction, delay aversion, reaction time variability, and emotional deficits. J Child Psychol Psychiatry 54: 619-27. doi:10.1111/ jcpp.12006
46. Schoemaker K, Mulder H, Deković M, Matthys W (2013) Executive functions in preschool children with externalizing behavior problems: a meta-analysis. J Abnorm Child Psychol, 41: 457-71. doi:10.1007/s10802012-9684-x
47. Bunford N, Evans S, Wymbs F (2015) ADHD and emotion dysregulation among children and adolescents. Clin Child Fam Psychol Rev 18: 185-217. doi: 10.1007/s10567-015-0187-5
48. Chiang H, Gau S (2014) Impact of executive functions on school and peer functions in youths with ADHD. Res Dev Disabil 35: 963-972. doi: 10.1016/j.ridd.2014.02.010.
49. Ardila A, Rosselli M, Matute E, Guajardo S (2005) The influence of the parents' educational level on the development of executive functions. Dev Neuropsychol 28: 539-560. doi:10.1207/s15326942dn2801_5
50. Arán-Filippetti V (2013) Structure and invariance of executive functioning tasks across socioeconomic status: evidence from Spanish-speaking children. Span J Psychol 16. doi:10.1017/sjp.2013.102
51. Hackman D, Gallop R, Evans G, Farah M (2015) Socioeconomic status and executive function: developmental trajectories and mediation. Dev Sci 1-17 doi:10.1111/desc.12246
52. Larsson H, Sariaslan A, Långström N, D'Onofrio B, Lichtenstein P (2014) Family income in early childhood and subsequent attention deficit/hyperactivity disorder: a quasi-experimental study. J Child Psychol Psychiatry 55: 428-35. doi:10.1111/jcpp.12140
53. Russell G, Ford T, Rosenberg R, Kelly S (2013) The association of attention deficit hyperactivity disorder with socioeconomic disadvantage: alternative explanations and evidence. J Child Psychol Psychiatry 5: 436-445. doi:10.1111/jcpp.12170
54. Skogli E, Teicher M, Andersen P, Hovik K, Øie M (2013) ADHD in girls and boys - gender differences in co-existing symptoms and executive function measures. BMC Psychiatry 13: 298. doi:10.1186/1471244X-13-298
55. Coghill D, Hayward, D, Rhodes S, Grimmer C, Matthews K (2014) A longitudinal examination of neuropsychological and clinical functioning in boys with attention deficit hyperactivity disorder (ADHD): improvements in executive functioning do not explain clinical improvement. Psychol Med 44: 1087-99. doi:10.1017/S0033291713001761
56. Albuquerque, G., Maia, M., França, A., Mattos, P., & Pastura, G. (2012). Processamento da linguagem no Transtorno do Déficit de Atenção e Hiperatividade (TDAH). Documentação de Estudos em Linguística Teórica e Aplicada, 28(2), 245-280. doi: 10.1590/S0102-44502012000200003
aPontifícia Universidade Católica do Rio Grande do Sul, Programa de Pós-Graduação em Psicologia - Porto Alegre/RS - Brasil
b Hospital Materno-Infantil Presidente Vargas, Departamento de Psiquiatria - Porto Alegre/RS - Brasil
Autor correspondente
Geise Machado Jacobsen
geisejacobsen@gmail.com
Submetido em: 21/09/2022
Aceito em: 11/10/2022
Contribuições: Geise Machado Jacobsen - Análise estatística, Coleta de Dados, Conceitualização, Gerenciamento do Projeto, Investigação, Metodologia, Redação - Preparação do original; Mirella Liberatore Prando - Coleta de Dados, Gerenciamento do Projeto, Redação - Preparação do original, Redação - Revisão e Edição; Gledis Lisiane Correa Luz Motta - Gerenciamento do Projeto, Redação - Revisão e Edição; Renata Kochhann - Redação - Revisão e Edição, Supervisão; Rochele Paz Fonseca - Conceitualização, Gerenciamento de Recursos, Gerenciamento do Projeto, Metodologia, Redação - Revisão e Edição, Supervisão.


artigo anterior voltar ao topo próximo artigo